
Disc Herniations: Why Size on Your MRI Doesn't Always Tell the Full Story (And Why That's Actually Good News)
- Jennifer Howard

- Mar 2
- 3 min read
Updated: Mar 10
You've just had an MRI for neck, arm, shoulder, or radiating pain. The report comes back with words like “large herniation,” “severe,” “significant compression,” or “extruded disc.” Your heart sinks: “This must be bad—will I need surgery? Is my spine ruined?”
That reaction is completely valid and understandable. This is something we see every week and scans can trigger real anxiety, especially with the sometimes brutal chosen words by the radiologist. But here's the reassuring truth from solid evidence: Size of disc herniation may not predict prognosis or recovery. [PMID: 41464802]
What the Research Actually Says
Words in reports matter, they shape how threatening pain feels which can open the "pain gate" wider (see my last blog piece on fear-avoidance) and keep you stuck in worry or avoidance.
Yet a strong 2025 study by Gül et al. (206 patients with cervical disc herniations, followed for 12 months) found no real link between herniation size and:
Baseline symptoms
Disability levels
1-year outcomes
The stats: odds ratio 1.010, p=0.323 (basically, size barely budged the needle on how things turned out). This is Level 2b/3 evidence which means, good quality to challenge the old idea that “bigger = worse.”
Inflammation often drives more of the symptoms than pure mechanical compression from size. The disc material can irritate nerves chemically, even if it's not huge. And crucially, many herniations improve naturally with time and conservative care.
Bigger Isn't Always Badder—Sometimes It's the Opposite
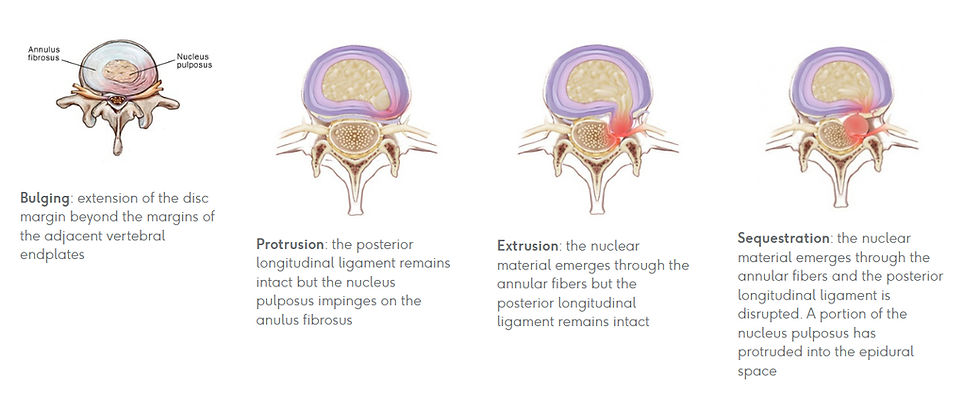
Paradoxically, larger or more extruded/sequestered herniations often regress better over time. Interestingly, this paradox arises because larger, more extruded or sequestered herniations are often more exposed to the body's immune system outside the disc's protective annulus, triggering a stronger inflammatory response that leads to resorption, e.g. via macrophages, neovascularization, and enzymatic breakdown. Smaller bulges or protrusions can linger longer because they're less exposed to that process.
Other studies back this:
Chiu et al. (2015) PMID: 25009200. A foundational systematic review (cited 305+ times): Spontaneous regression rates:
96% for disc sequestration
70% for disc extrusion
41% for disc protrusion
13% for disc bulging
Complete resolution was also higher: 43% for sequestrated vs. 15% for extruded.
Conclusion: Patients with extrusion and sequestration had a significantly higher chance of regression than those with bulging/protruding discs.
Rashed et al. (2023) PMID: 37486886. Systematic review and meta-analysis (updating Chiu): Probabilities:
93.0% for sequestered
70.4% for extruded
52.5% for protruded
13.3% for bulging Larger baseline volume (e.g., 1260 mm³ vs. 1006 mm³) and transligamentous/extruded types predicted better regression.
The Takeaway
Your scan is a snapshot of anatomy, not a predictor for pain, disability or future. Many people live active lives with "big" findings that never caused issues and plenty with "small" ones feel significant pain until inflammation calms.
Breaking the Worry Cycle
If scan anxiety or neck/arm pain is weighing on you, conservative steps work for most:
Gentle hands-on care: Manual adjustments, mobilisations, dry needling, remedial massage and more, reduce guarding, ease nerve irritation and dial down inflammation often bringing quick relief without forcing movement.
Education & mindset shift: We go through your report together, reframing it so it feels less threatening. Pain is protective and very real, but often more alarm than permanent damage.
Graded movement: Start small and safe (gentle neck stretches, walks), build confidence progressively. Avoid total rest, movement helps close the pain gate and supports natural regression.
Other advice: Address stress, sleep, posture, things that influence inflammation and recovery more than size alone.
When to check further: Severe weakness, numbness, or no progress after weeks may need specialist review, but that's not the default path.
While most people see significant improvement without surgery or injections, a smaller group may need more advanced options or ongoing management. That doesn’t mean hope is lost — it means finding the approach that fits your body and circumstances.
You're not defined by your MRI/CT/X-ray. Inflammation can settle, fear can fade and function return, in many cases.
Disclaimer
These are general insights based on common patterns in research and clinic experience. Everyone’s body and situation is unique — some recover quickly, others take longer or need different paths. If your pain is persistent or worsening, always seek personalised guidance. This article is general information only — it is not a substitute for personalized medical advice.



Comments